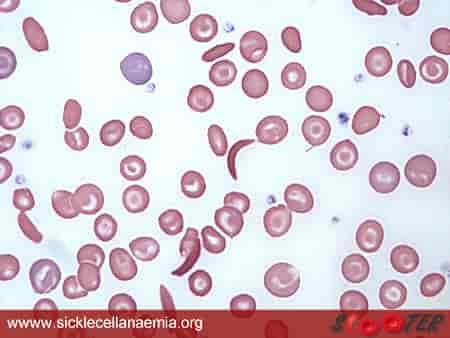
Sickle Cell Disease (SCD) is a genetic disorder that affects hemoglobin, the protein in red blood cells responsible for carrying oxygen. Instead of the normal bi-concave shape, red blood cells assume a sickle or crescent shape, heightening their fragility and hindering efficient oxygenation. Because people with sickle cell already are suffering the effects of decreased oxygen in the blood, symptoms varying in degree of pain from headaches, shortness of breath, agonizing pain akin to stabbing sensations, and other associated diseases lung problems are commonplace. While such challenges are well-documented, there’s a silent threat that often goes unnoticed – the impact of certain behaviors such as smoking on individuals living with Sickle Cell Disease.
The challenges faced by individuals with Sickle Cell Disease (SCD) are significantly exacerbated by smoking. This detrimental effect is primarily due to smoking’s introduction of carbon monoxide into the bloodstream, which substantially reduces its oxygen-carrying capacity. Consequently, individuals are at a heightened risk of experiencing painful episodes.

Smoking is a significant risk factor for various health issues in individuals with Sickle Cell Disease (SCD), particularly contributing to the development of complications such as Acute Chest Syndrome. It is crucial to emphasize that both active smoking and exposure to environmental tobacco smoke (secondhand smoke) are linked to a rate of Acute Chest Syndrome(ACS) episodes that surpass twice the frequency observed in individuals with no smoke exposure (Cohen et al., 2010, Gray et al., 1991; Young et al., 1992; Sadreameli et al.,2016). ACS, characterized by sudden chest pain, fever, and respiratory distress, stands as a primary cause of illness and hospitalizations among SCD patients, second only to recurrent pain episodes. ACS 25 % of all deaths in patients with SCD (Gray et al., 1991)
Additionally, both active and secondhand smoke can contribute to heightened inflammation in blood vessels, induce the aggregation of blood cells, and enhance the inner lining of blood vessels’ susceptibility to attracting and retaining substances, thereby elevating the risks of blockage. There is also a higher risk of contracting pneumonia. Complications from pneumonia include respiratory failure and even death. The elevated mortality rate among young adults with SCD points to the fact that both smoking and current asthma are significant predictors of mortality. (Knight-Madden et al., 2013)
Why smoke? Nicotine has a mellowing effect on individuals, masking pain perception and temporarily causing anxiety relief, making it an attractive method for individuals with SCD to cope with their pain. Because smoking increases pain, the recurrent pain serves as a significant motivator for continued smoking, creating a vicious cycle. The harmful cycle established by smoking intensifies pain, leading to increased stress and prompting individuals to resort to smoking as a coping mechanism. SCD patients should be taught skills to break this vicious cycle.

The complex relationship between smoking and Sickle Cell Disease (SCD) underscores the urgent need for targeted interventions and increased awareness programs, specifically designed to address the health risks smoking poses to individuals with SCD. The crucial strategy involves empowering the SCD community with effective coping mechanisms and promoting widespread knowledge about the negative impact of smoking on their health. Breaking the destructive cycle initiated by smoking, especially given the context of recurring pain, is a critical step in improving the overall well-being of this group. Additionally, fostering engagement with healthcare providers and encouraging participation in support groups not only provides personalized guidance but also cultivates a community where shared experiences and mutual support pave a more effective route toward cessation of smoking.