Join us July 21st for a Health and Wellness Celebration designed to end the stigma around HIV.
This community health and wellness celebration will bring resources, fun and connection to the community. While ending HIV stigma will be our focus, we brought together a collection of community partners invested in the community from all ranges and reaches! With live entertainment, health services, games, and more want to celebrate GOOD HEALTH with our Grand Rapids family.
The event is FREE and no registration is required.
GRAAHI’s director of research, Andrae Ivy serves on the board of the Black Leadership Advisory Council (BLAC). At GRAAHI we’re proud to join with BLAC in order to support legislation to break down systemic barriers. Read the full news provided by BLAC, and click HERE to read more about the organization and the 11 recommendations they have made to the State of Michigan.
Members of the Black Leadership Advisory Council (BLAC) joined Gov. Whitmer, Lt. Gov. Gilchrist and Sen. Sarah Anthony to celebrate the signing of the CROWN (Creating a Respectful and Open World for Natural hair) Act, which bans hair discrimination and removes barriers to Black Michiganders achieving economic prosperity.
“I am proud to sign … bipartisan legislation alongside Senator Anthony to end hair discrimination in Michigan,” said Governor Whitmer. “The CROWN Act will address hair discrimination Black Michiganders face at work, at school, and elsewhere. Black Michiganders must be able to wear their natural hairstyles however they choose and not feel forced to change or straighten their hair for interviews, work, or school. We know that 44% of Black women under the age of 34 have felt this kind of discrimination before and I am proud that we are taking an important step forward today to make our state more equitable and just. Let’s keep working together on our comprehensive Make it in Michigan vision to build a state where every Michigander can work, live, and raise a family.”
Black Leadership Advisory Council Support & Recommendations
The CROWN Act was one of 11 policy recommendations BLAC offered to Gov. Whitmer in their 2022 report based on subject expert presentations and other forms of research and analysis.
“From bias in job recruitment to natural hairstyles being restricted in schools, our community is subjected to race-based discrimination every day, and the CROWN Act shows Black Michiganders – and the world – that we deserve equal opportunities and the freedom to show up as our most authentic selves,” said BLAC co-chair Dr. Donna Bell. “We applaud Gov. Whitmer and the legislature for bringing the CROWN Act to Michigan and banning hair discrimination in our state.”
“Following my work with Kent County to pass local policies to ban race-based hair discrimination, I am overjoyed to know all Black Michiganders will now receive these protections,” said BLAC co-chair Robert Womack. “The Black Leadership Advisory Council applauds our state leaders for passing this meaningful legislation and adding Michigan to the growing list of partners in this national movement.”
This past 2022-2023 school year, the Grand Rapids African American Health Institute (GRAAHI) Pathways program has partnered with the Grand Rapids Public Schools (GRPS), University Preparatory Academy and Ottawa High School and colleges and universities to provide students who are interested in a healthcare track the opportunity to complete a college tour focusing on college/university health programs. The hands-on experience that students were able to garner from the college tour created a lifelong impact.
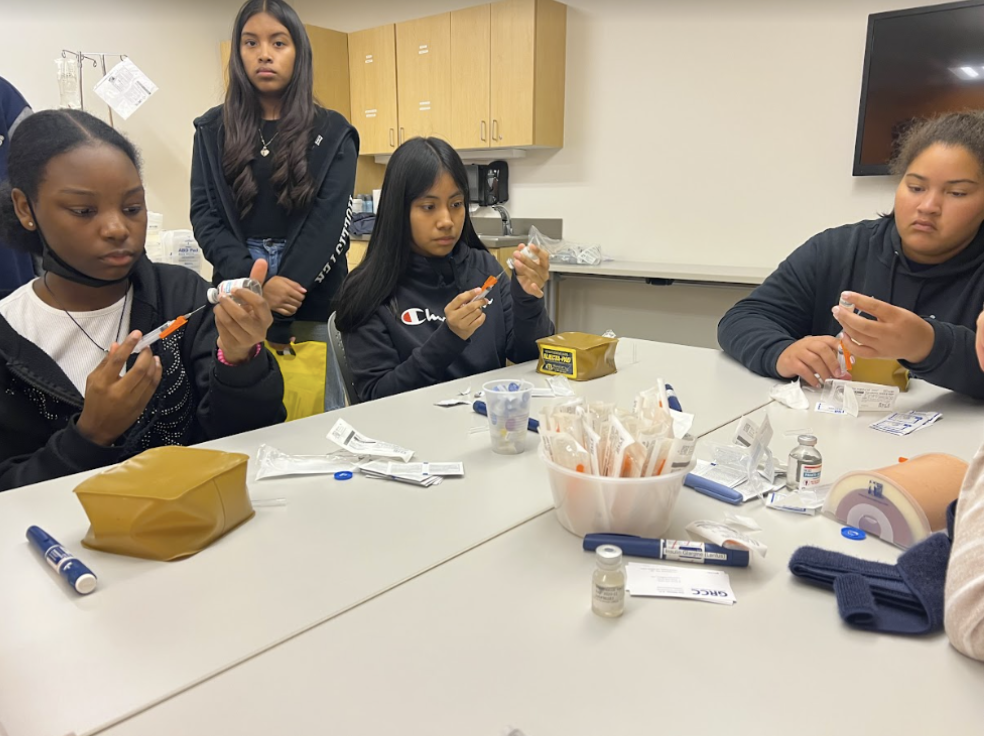
In October 2022, Grand Rapids Community College kicked off the college visits by having students walk through a series of lab simulations that include the following fields: medical assisting, nursing, and occupational therapy. Students were able to use healthcare equipment such as syringes, lab dummy patients, stethoscopes, and various therapy equipment. What was important about the GRCC visits were the personal journeys that were told by the health professionals regarding their healthcare journey.
In January 2023, Davenport University hosted a college visit that focused on health activities: nursing and research query. Students had a chance to interact with equipment as well as a data set and reviewed data mining tools. Students’ various activities for the data set reviewed the rudimentary data sets as well as complex data such as music playlists. The information provided was relatable to students and engaging. Davenport University provided a unique opportunity for the student nurse association to present as well as have a presentation on their admission process.
In March 2023, Ferris State University hosted a college visit that focused on nursing and dentistry. Students were able to walk through the history of dentistry, put teeth in a mold based on the anatomy of teeth, walked through a live dentist clinic, and interact in the nurse lab simulation space. The students had a chance to talk with a student and their experience of Ferris as well as hear about their various health programs.
The unique experience that each college/university sparked student comments of wanting to continue the learning opportunities, wanting to see more on the campus, and enjoying presentations by students. The real opportunity that the colleges and universities are providing to each student is the opportunity to be excited about attending and being a part of a community that supports them in a healthcare track as well as getting students comfortable with being on campus. Having a sense of familiarity on campus and seeing the culture of the campus in the healthcare programs helps students to reimagine themselves on campus and ignites a sense of belonging prior to attending college. GRAAHI is truly grateful to GRPS school administrators, participating colleges and universities, and students and families that have participated in these healthcare college tours. The tours are truly making a difference in the joint communities we serve. GRAAHI looks forward to next year as we continue the healthcare college tours with a Fall 2023 kickoff with Grand Valley State University.
By Vanessa Greene for the Grand Rapids Business Journal – Published February 17, 2023
It’s no secret that historically, health care outcomes for Black people and other non-white Americans have been an area of concern.
These numbers, from longstanding systemic inequities in the health care system, social determinants such as a lack of accessible health care facilities in some communities, to outright discrimination, can leave Black residents less likely to trust doctors and seek proper care. This last point was most evident during the height of the COVID-19 pandemic, when more Black residents were dying in part due to this distrust of the medical establishment.
At the Grand Rapids African American Health Institute, we recently undertook a much more local approach to this issue and have analyzed state data to showcase the severity of the disparities right here in our backyard of Kent County.
County-level disparities
Led by our research coordinator Andrae Ivy, MPH, we dove into state health care data from 2014 through 2020, examining 17 key health trends — from diabetes and obesity, to cancer, infant mortality and teenage births — and how they impacted Black, white and Hispanic residents in Kent County.
What quickly emerged was a troubling pattern. Among the biggest Kent County trends were:
15.1% of Black residents have diabetes vs. 10% of white residents
Obesity rates were 41.6% for Black residents, compared to 28.5% for white residents and 30.1% for Hispanic residents.
Heart disease mortality rates continue to climb for Black residents, reaching a new high of 541.3 per 100,000 residents. Stroke mortality also grew significantly from 2017 to 2020.
10.2% of Black residents could not see a doctor due to health care costs vs. 8.8% for white residents.
Asthma rate for Black residents was 19% vs. 14.1% for white residents.
Both the prostate cancer rate (135 per 100,000 men) and lung cancer rate (75.9 per 100,000 residents) for Black residents were significantly higher than rates for white residents.
Infant mortality rate was 13.8 per 1,000 births for Black residents, nearly triple the 4.8 per 1,000 births rate for white residents.
Teenage birth rates were much higher for Black residents (32.3 per 1,000 females ages 15-19) and Hispanic residents (27.3), compared to the 7.7 rate for white residents.
Medical debt due to out-of-pocket costs is another major obstacle. According to a 2022 survey of Michigan residents by Epic-MRA and the advocacy group Consumers for Quality Care, among Black voters that have had their household finances seriously affected by medical debt, 80% say they’ve had medical bills go into collections.
Also, 65% of Black voters expressed concern that health care costs will be negatively impacted by long-term effects of COVID-19 in Michigan, compared to 58% of the state’s population overall. And 69% of Black Michiganders are concerned about expected impending loss of health care coverage expanded during the pandemic through the Affordable Care Act, compared to 51% of the state’s population overall.
Addressing inequities
While there is not one easy answer that will close these gaps in health care for Kent County’s Black residents, one thing is clear. Without major improvements to the systems surrounding access to health care in communities of color, these disparities in West Michigan and beyond will continue to persist.
Between changes at insurance companies to improve affordability of health care, increased state and federal support, and significant local community efforts, policymakers must prioritize implementing policies that improve health outcomes in the Black community.
Compared with whites, members of racial and ethnic minorities are less likely to receive preventive health services and often receive lower-quality care. They also have worse health outcomes for most conditions. To combat these disparities, legislators and health care professionals must explicitly acknowledge that race is a factor in health care.
Although the majority of individuals have at least one full-time worker in the family across racial and ethnic groups, people of color are more likely to live in low-income families that do not have coverage offered by an employer and have difficulty affording private coverage. According to a recent study by the Kaiser Family Foundation, the ongoing gaps in coverage for people of color could further widen the coverage gaps they already face and, in turn, exacerbate broader disparities in health and health care. With this in mind, efforts to increase insurance coverage and make health care affordable are crucial.
My organization works every day to educate the public on their health care rights and how to navigate the system, while also teaching preventive health care measures, as we work to help change these statistics. But officials at the city, state and federal levels, as well as health care systems and insurance companies, must recognize the serious inequities this research has exposed and work to address them. Improving disparities requires a collective effort across many systems and organizations.
Some examples include working to address key social determinants that can lead to poor health, offering more accessible and affordable health care options in communities of color that lack them, diversifying the health care workforce, proactively connecting patients with supportive social services and eliminating inequities in the quality of care. Additionally, it is important to monitor and document efforts toward reducing health disparities to determine what’s working.
If we’re ever going to deliver a realistic chance at equal access to quality health care for all residents of Kent County, we must work together vigorously as if our own lives depend upon it.
Health Careers Club introduces elementary students of color to occupations
By Erin Albanese February 15, 2023 | School News Network
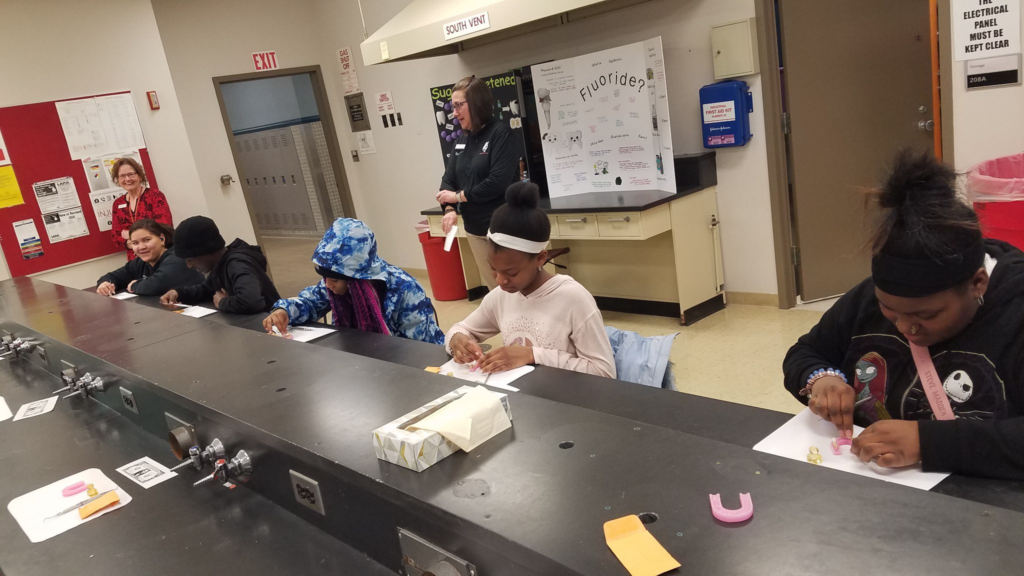
Students engage in conversation and an activity arranging certain food on a plate with Kent County registered dietitians
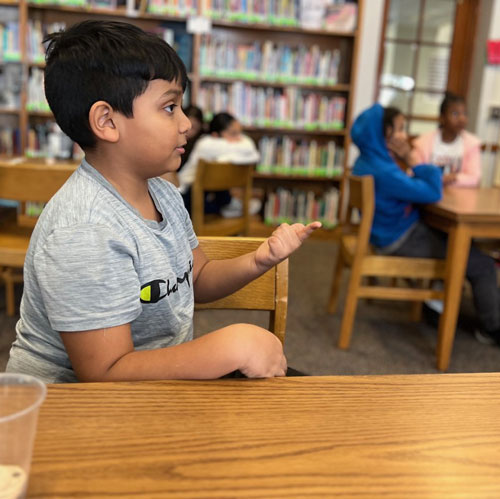
Third-grader Alfredo Rajas examined clues as to why people were falling ill with respiratory symptoms in Milwaukee and Chicago.
“Fifteen people have been visiting the emergency room and have been having trouble breathing lately,” he said, catching on quickly to the role of a health investigator. “They have fevers and other stuff that make them feel really bad.”
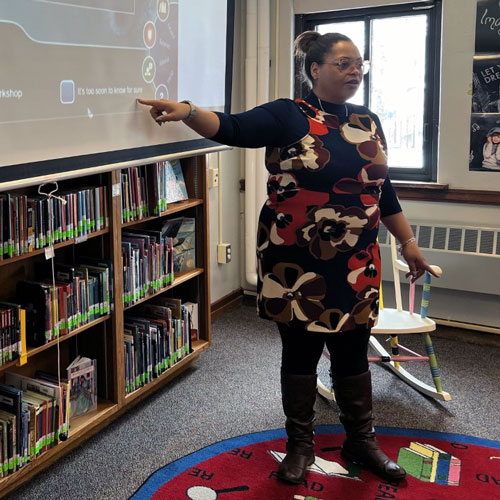
Brandi Berry, program supervisor for the Kent County Health Department, explained what that could mean.
“When you have more than three people with the same symptoms, you have the potential for an outbreak,” she said.
A group of Stocking Elementary students were playing a game with Berry to introduce them to careers in public health, one of several health care fields they are learning about this school year as part of Pathways to Healthcare Careers, a program offered by the Grand Rapids African American Health Institute.
From left, students Janelle Whitley and Amarianna Richards listen to details of a simulated outbreak
The game, Solve the Outbreak, on the Centers for Disease Control and Prevention website, presents information and clues, and demonstrates how “disease detectives” investigate outbreaks.
“The Health Department helps everybody,” Berry told students. “We make sure that you have clean water, that the air is good. We make sure everybody gets their shots and that you’re healthy.”
‘We want students to see themselves in the doctor’s coat.’
— Stacey Baker, program coordinator for Grand Rapids African American Health Institute
But, she explained, some things that affect people’s health, like COVID-19, require investigation because they are dangerous. That is the role of a health investigator.
“Outbreaks happen in the world. We just had an outbreak – COVID. When something like that happens it can be very dangerous. We don’t want outbreaks.”
Third-grader Alfredo Rajas talks through clues in the game ‘Solve the Outbreak’Brandi Berry, the program supervisor for the Kent County Health Department, introduces students to public health careers.
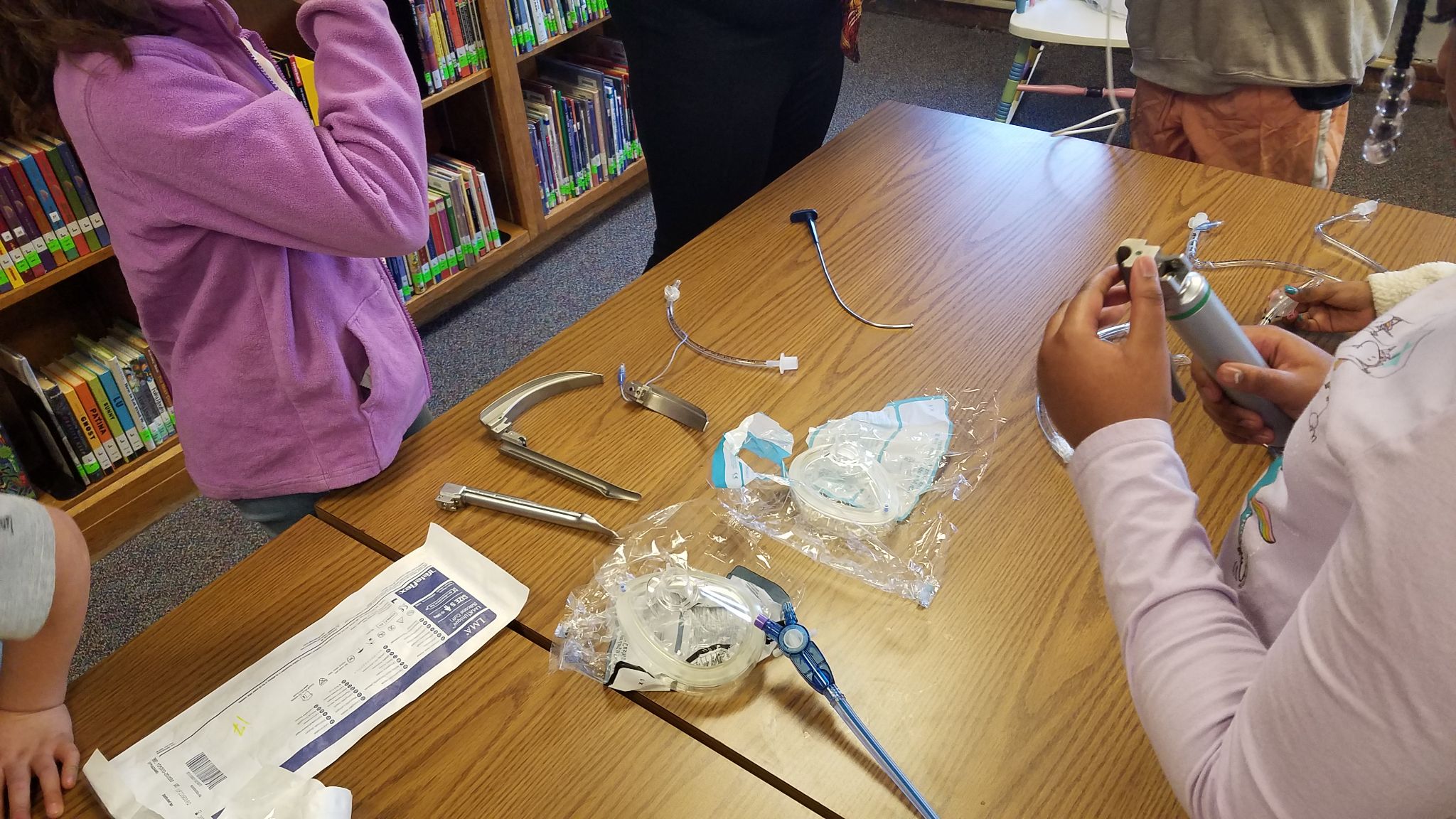
Students spend an hour every Monday in Pathways and have learned about occupational therapy, phlebotomy, dietetics and nursing by meeting professionals and getting to see and touch equipment.
The goal is to expose children of color to health care careers while helping boost their academics, said Stacey Baker, program coordinator for GRAAHI.
“We want students to see themselves in the doctor’s coat or in the shoes of other health care professionals,” Baker said. “We want them to see a variety of health care occupations to grow and expand their knowledge base.”
People of color are drastically under-represented within the healthcare field, he said. According to 2017 and 2019 data from the U.S. Department of Health and Human Services and the National Center for Health Workforce Analysis, whites make up the majority of the U.S. medical workforce, at 64.4 percent; compared to Hispanics, at 16.1 percent; Blacks or African Americans, at 11.6 percent; and Asians, at 5.3 percent.
Having people of color in healthcare professions improves outcomes as well, Baker said. “Studies have found that when patients of color see health care workers of color they tend to do better in terms of their health overall.
Pathways pairs academic tutoring in reading and math — through Sylvan Learning — with the career presentations, equipping students with academic skills to eventually pursue careers. Baker said that’s an important piece to the program.
“They need to be academically proficient in terms of the sciences.”
The program is also offered at Grand Rapids University Preparatory Academy, a middle and high school, and Ottawa Hills High School. Along with seeing health care professionals in action, the high school program involves tours of college campuses and program visits.
Donovan Jones takes part in the investigation
Inspiring Young People
By using their sleuthing skills in the game, Stocking students figured out that the outbreak was caused by anthrax. A musician who visited Africa had returned with the deadly bacteria on his drums. When he played at a concert in Chicago, beating the drums caused the anthrax spores to disperse in the air and infect the audience.
Alfredo enjoyed the investigation and said he’d like to be a health investigator one day.
“The research — you get to find out clues — it’s like a scavenger hunt,” he said. “I want to keep the community safe and I don’t want anyone to get a bad illness.”
Thanks to a $1 million American Rescue Plan Act (ARPA) grant awarded by Kent County, the Grand Rapids African American Health Institute (GRAAHI) will expand and enhance programming aimed at reducing health disparities within the county’s BIPOC communities. Founded in 2002 in reaction to a Kent County Health Department community needs assessment, the grassroots organization has leveraged community input and collaborations with other organizations to address disturbing racial disparities in maternal and infant mortality, diabetes, access to mental and medical health care and more.
“That survey showed daunting, glaring disparities — more than the community had anticipated,” says Vanessa Greene, GRAAHI CEO. “Disparities are not just a result of treatment experiences. Eighty percent of health disparities are a result of social determinants — where people live, which determines where they go to school, and then that determines their ability to access resources and higher education, which then informs what type of job they’re going to get. The type of employment determines what type of health insurance that they have.”
Some of the grant money will help fund GRAAHI’s health navigator programs, which focus on maternal infant health and mental health. GRAAHI’s mental health navigators aim to connect at least 500 African Americans with mental health services to address needs exacerbated by the COVID-19 pandemic. Navigators working with expectant mothers aim to reduce BIPOC maternal and infant mortality and morbidity. A 2020 Kent County Community Needs Assessment found that nearly twice as many Black babies here died in their first year of life than white babies (8.1 per 1,000 compared to 4.5 per 1,000 live births). Similar disparities exist across the U.S. Research has determined that racism-induced stress is a major root cause.
“We still have mothers who are not highly engaged in prenatal care, who don’t have the comfort level [with their provider],” Greene says. “Community health navigators help them through that process and walk alongside them. We want to be really intentional about supporting pregnant women and making sure that they understand every stage of their pregnancy and have the resources to help them navigate that process.”
“When people come in, it’s important for them to see faces that look like them,” Greene says. “Having increasing diversity in the health care sector is important for [those working in health care to understand] how cultural relevance and affirming treatment impacts the overall attitude and trust level of the patient. The other factor, COVID, created a lot of shifts in terms of people leaving the health care system. There’s a shortage in almost every [health care] field.”
GRAAHI also plans on expanding its Restoring Health program that serves Kent County’s older adults who were adversely impacted by COVID-19 and now face deteriorating health due to chronic conditions, poor nutrition, lack of physical activity, or social isolation. In addition, GRAAHI plans to enlist more than 100 repeat blood donors to help sickle cell patients survive that disease, which is prominent within the Black community.
“We’re nowhere close to achieving all of our goals, but we are really excited about the strides that we’re making and the systems that we have in place,” Greene concludes. “We do anticipate seeing even greater results and impact with this funding we’re receiving from the county.”
Written by Estelle Slootmaker, Development News Editor Photos courtesy GRAAHI
Article is copied from Rapid Growth Media – https://www.rapidgrowthmedia.com/devnews/0130graahi.aspx
Andrae Ivy, MPH | GRAAHI’s Director of Research | February 2023
On January 27th of 2023, the world watched yet again as a Black man named Tyre Nichols was viciously beaten and harassed by a group of police officers in Memphis, TN. The images, words and violence in this video were terrifying to watch, as the officers seemed determined to end this
young man’s life following a routine traffic stop. After being violently punched, kicked and tasered, Mr. Nichols would eventually slump to the ground, blood running down the side of his swollen and distorted face onto the cold pavement. The officers showed no signs of treating Mr. Nichols like a human being before, during or after the attack, as they casually shared excuses and lies to justify their violence. The grotesque injuries Mr. Nichols suffered from the beating can also be viewed, as he laid lifeless in a Memphis hospital room with a face reminiscent of Emmett Till’s. Unfortunately, Mr. Nichols would eventually succumb to his injuries and lose his life three days later. Upon release of the video, five of the officers involved in the incident were fired. That following Monday on January 30th, a sixth officer was fired in connection with the beating. This traumatic event is all too familiar for Blacks or African Americans who are often reminded of their fragile and devalued nature in the face of police officers. Blacks are tired of this state-sanctioned treatment and need tangible protections and anti-hate policies to prevent such attacks from reoccurring.
From Rodney King to Sandra Bland to George Floyd to Breonna Taylor to Tamir Rice to Atatiana Jefferson to Patrick Lyoya and so many others, the deaths of Blacks or African Americans in the presence of police officers are commonalities that plague the hearts and minds of not only the victims and their families, but also those who share a similar phenotype across the many cities and states in this country and across the world. According to Mapping Police Violence, Blacks in America are nearly three times more likely to be killed by police officers compared to whites, resulting in 254 Black deaths in 2022. In addition, this study found that 100 out of 100,000 Black men and boys will be killed by police officers during their lifetime compared to 39 white men and boys. Since Blacks as a whole collectively share the grief and trauma of these deaths, it’s important for Blacks and society to better understand the cumulative effects of these unethical actions on the mental, physical and emotional health of the entire Black population. Several studies have investigated the impact of traumatic events, such as police brutality and racism, on the overall wellbeing of Blacks. One study in 2018, led by Dr. David Williams, found that the killing of an unarmed Black person by a police officer resulted in many days of poor health for Blacks in that state for the next three months. Another study found that Blacks and other non-white groups were more likely to report police victimization, in which that victimization was significantly linked to psychological distress and depression. In a more robust study, researchers found that the constant threat of police violence, the actual acts of police brutality, and the aftermath of these events have a collective and “allostatic load” effect on the mental health of those victimized along with those who identify racially or culturally with said victims. In addition, this study also determined that the effects of police brutality mirror the effects of racism
occurring within many facets of society such as housing, education, employment and health care.
In this interesting study, Black drivers in America were nearly 20% more likely to be stopped by police officers and nearly twice as likely to be searched compared to their white counterparts. When being confronted by police officers, many Blacks run and flee, which is viewed by some as an indicator of guilt. Many Blacks know the history of this country and the unequal treatment with police officers and the justice system, even when no wrongdoing has occurred. In 2016, the Massachusetts (MA) Supreme Judicial Court showed support for this reality regarding a Black man in Boston who was wrongfully profiled during a police investigation. The MA Supreme Court stated, “The finding that Black males in Boston are disproportionately and repeatedly targeted for FIO [Field Interrogation and Observation] encounters suggests a reason for flight totally unrelated to consciousness of guilt. Such an individual, when approached by the police, might just as easily be motivated by the desire to avoid the recurring indignity of being racially profiled as by the desire to hide criminal activity.” This statement by the MA Supreme Court basically means that Black men running from police officers is understandable due to the fact that Black men are more likely to be racially profiled. Their statement also confers that some Black men simply run to escape the indignity of being racially profiled and a potential victim of police brutality, and that this shouldn’t indicate any form of guilt on their part. This is important to note when thinking about Tyre Nichols who decided to run in an attempt to reach his mother’s home, just sixty yards away. Unfortunately, he was unsuccessful.
Typically, police brutality against Blacks usually involves white officers. In Tyre Nichols’ case, the officers involved were mainly Black, indicating that Black officers can also possess and demonstrate hate, bias and prejudice towards Black life. Such behavior is repulsive no matter the person’s background, and justice should be served no matter the officer’s race. This fact reinforces calls to investigate police departments, unions and officers to determine their ability to serve and protect the community without bias, hate and prejudice. If not, more innocent lives will be lost. On another note, these acts of police brutality from some officers stain the image and reputation of all officers, even though this behavior isn’t indicative of all officers. Like many citizens, many police officers also expressed their dismay with the vile behavior displayed by the officers in Mr. Nichols’ case and many other cases of police brutality, showing that all officers can’t be blamed for the actions of some. The Grand Rapids African American Health Institute (GRAAHI) is dedicated to increasing health equity for Blacks or African Americans in the Grand Rapids community. These acts of violence against Black bodies impact our mental and physical health. We are deeply troubled by the death of Tyre Nichols and so many others. Even though these officers were swiftly charged, many systematic changes, such as anti-Black hate policies and protections, are needed to revamp and rebuild the justice system and the consciousness of Americans, so a person’s life isn’t deemed less valuable because of the color of their skin.
We at GRAAHI offer our sincerest thoughts and prayers to the family of Tyre Nichols.
This January, National Blood Donor Month, GRAAHI follows in the footsteps of two heroes for life, Rev. Dr. Martin Luther King, Jr., and Dr. Charles Richard Drew, by joining with Versiti to hold a Blood Drive at Brown Hutcherson Ministries.
In the 1940s, Dr. Charles Drew laid the groundwork for today’s modern blood donation program through his innovative work in blood banking. The Red Cross blood bank program began in 1940, under the leadership of Drew who became the organization’s first medical director in 1941.
“He was a surgeon, educator, scientist and the first African-American blood specialist who helped shape the blood services industry. His legacy is far-reaching and we hope this drive helps educate the community about the need for a diverse blood supply,” said Vanessa Greene, CEO of the Grand Rapids African American Health Institute.
Why is an ethnically diverse blood supply important?
Because blood type is inherited, a compatible donor is often someone of a similar ethnic background. Diversity in donation is important for improved patient outcomes, as rare and uncommon blood types are often found in similar ethnic populations.
For example, sickle cell patients may require chronic blood transfusions to treat their disease, Since 44% of African Americans have Ro blood, providing matched Ro blood to sickle cell patients may provide a safer blood transfusion. Patients are less likely to experience complications from blood donated by someone with a similar ethnicity.
Become a Hero for Life and feel the good benefits of supporting your community. Join us January 21st from 9:30am to 1:30pm at Brown Hutcherson Ministries, 618 Jefferson Ave SE, Grand Rapids, MI, 49503. GRAAHI seeks to create a welcoming and safe environment with a team focused on supporting your needs as you donate.
Every pint can save 3 lives!To sign up to donate, and learn more about Dr. Drew, go to graahi.com/giveblood.
Grand Rapids, Mich. (Dec. 19, 2022) – The Grand Rapids African American Health Institute (GRAAHI)announced today it has received a $1 million grant through the federal government’s American Rescue Plan Act (ARPA). GRAAHI was one of 30 grant recipients out of a total of 300 area applicants selected to receive funding by Kent County.
“We are pleased the Kent County administration and commission recognizes the important work GRAAHI provides in this community and has chosen to support our future efforts,” said Vanessa Greene, GRAAHI CEO. “As the leading health equity advocate for African Americans in greater Grand Rapids, we plan to use this federal funding to increase health-related resources for our residents and build on our efforts to make access to healthcare more equitable for all.”
Investing in new and existing mental and physical health programs for local communities was consistently described as “the first priority” in federal, state, and Kent County’s plans for spending ARPA funds. As part of its application process, GRAAHI presented plans to expand our services and impact in these areas. Specifically:
Expanding and enhancing mental health navigation services for Kent County’s BIPOC residents.
PROGRAM GOAL/Impact: At least 500 African American residents of Kent County whose mental health needs have developed or been exacerbated as a result of the COVID-19 pandemic will be connected annually to mental health services to regain their optimallevel of physical, mental, emotional, and social functioning during the 4-year project period.
Expanding and enhancing the representation of BIPOC professionals in Kent County’s healthcare workforce.
PROGRAM GOAL/Impact: Increase representation of African American and Latinx individuals in the Kent County healthcare workforce by engaging an additional 200-300 students annually from 2023-2026.
Launching a maternal and infant health community navigation program to serve BIPOC individuals and families in Kent County at high risk of disparate pregnancy outcomes.
PROGRAM GOAL/Impact: Significantly reduce the high and disparate rates of maternal and infant mortality and morbidity from all causes in Kent County’s BIPOC communities.
Expanding and enhancing the Restoring Health program that serves senior citizens in Kent County whose health deteriorated as a result of the social isolation and medical experiences they endured during the COVID-19 epidemic.
PROGRAM GOAL/Impact: To serve 300 or more BIPOC adults 65 and older in Kent County each year who were adversely impacted by COVID-19 and/or whose health and wellbeing are now deteriorating or are at risk of deteriorating as a result of chronic conditions, poor nutrition, lack of physical activity, and/or social isolation.
Organizing and directing county-wide blood drives with a focus on sickle cell patients.
PROGRAM GOAL/Impact: Expand our outreach to over 100 repeat blood donors in Kent County annually, each donating four times per year, resulting in over 1200 lives saved.
“This grant is both an investment in our community’s future health and a validation of the past work by GRAAHI over the past 20 years,” said Paul Doyle, GRAAHI Board Chair. “Since being established in 2002, GRAAHI has worked to improve access to healthcare for marginalized populations, provided health services to uninsured residents and improved the overall wellness of Black and Brown populations in the greater Grand Rapids area. This grant validates our work and sets the foundation for an even greater impact in the coming years.”
Recently our CEO, Vanessa Greene, spoke with Shelley Irwin at WGVU. Listen here.
Join us December 17th as we co-host a FREE Christmas shopping opportunity for families in need. In a time of residual and onging challenges with a pandemic and rising costs, we understand that creating an abundant holiday can be additional stress to your mental health. That’s why we are supporting Meaning in Colors in creating this fun community-centered shopping event. The heads of families can shop for their family members from a stock-pile of donated goods! No kids are allowed at the event as this is meant to be a suprise for them! (Hello Santa!)
Currently we are signing up families to shop at: FAMILY SIGN UP
We’re also inviting community members and organizations to donate new items to our shop. And we’d love to have additional hands on that day with friendly volunteers. To make a donation or volunteer, email us at: MIC.info@MeaningInColors.org
We’re honored to co-sponsor this event with Meaning in Colors, a local nonprofit that strives to support education and housing for our community members. Collaborations like this mean we’re tackling the social determinants that impact the health of our black and brown communities.